
A rare disease solves the mystery of a common drug
An ultrarare muscle disease caused by HMGCR mutations illuminate statins' controversial side effect

Happy Friday! A recent paper published in the Journal of Experimental Medicine reminded me again of rare disease and drug development. In the paper, the authors report the first cases of complete deficiency of an immune-related protein called PD-L1 (programmed death ligand 1). PD-L1 is one of the targets of a major class of anticancer drugs called ‘checkpoint inhibitors’, which bring billions of dollars in revenue for pharma companies every year. The PD-L1 human knockouts recapitulate one of the many autoimmune adverse effects caused by checkpoint inhibitors—type 1 diabetes. I wrote a small post recently on this. Perhaps, it can be a topic for a future post. But reading this paper reminded me of a Twitter thread that I wrote a year ago on a rare recessive muscle disease caused by deficiency of HMG CoA reductase, the target of another popular class of drugs—statins. I have highlighted this paper on my 2023 roundup and have told the story in the 2023 year-end episode of The Genetics Podcast. Still, it deserves to be a standalone post in my Substack. So, I picked it for this week’s From the Twitter archives post.
From the Twitter archives

A major adverse effect of statins is muscle myopathy (known since 1980). Human genetics have recently shed light on this association. Two independent teams have now discovered that recessive mutations in HMGCR cause a severe form of muscular disease in humans.
HMGCR codes for HMG CoA reductase, which converts HMG-CoA to mevalonate, a rate limiting step in the cholesterol synthesis. Statins act by inhibiting HMG-CoA reductase.

Statins were discovered in the 1970s by a Japanese scientist, Akiro Endo. The statins are, according to WSJ, "the first in a class of medicines that today brings $25 billion a year to pharmaceutical companies." Yet, Endo derived no financial benefit from his discovery. Michael S. Brown and Joseph Goldstein, who got Nobel Prize for cholesterol related work, famously said "The millions of people whose lives will be extended through statin therapy owe it all to Akira Endo".
Refer to this fascinating WSJ article on Endo's story: "How One Scientist Intrigued by Molds Found First Statin". Endo’s childhood fascination on the discovery of penicillin by Alexander Flemming was a major inspiration behind the statin discovery. Fascinatingly, the fungal mold that led to the development of breakthrough medicine was found on the rice grains that Endo purchased from a small grocery shop in Kyoto.
Coming back to our main topic, it turns out that the very first human, an 18 yr old female, who received statin developed severe myopathy to the point she was unable to walk. After the drug was discontinued, the patient made a full recovery.

After this incident, the company didn’t want to continue the trial. But Endo and his colleague (Akira Yamamoto) continued the trial, but this time giving smaller doses and achieved a 27% drop in blood cholesterol, proving to the company that the drug works and is safe in smaller doses.
As the statins got used widely across the world, it became apparent that muscle weakness and pain is indeed a common adverse effect, reported by ~30% of the users. If statins really cause muscle pain has always been a topic of debate among the clinicians, even today. Even if that was true, the underlying mechanism remained elusive.
Now, more than four decades later, two independent groups of researchers have encountered patients with a rare muscular disease that turned out to be caused by biallelic mutations in HMGCR.
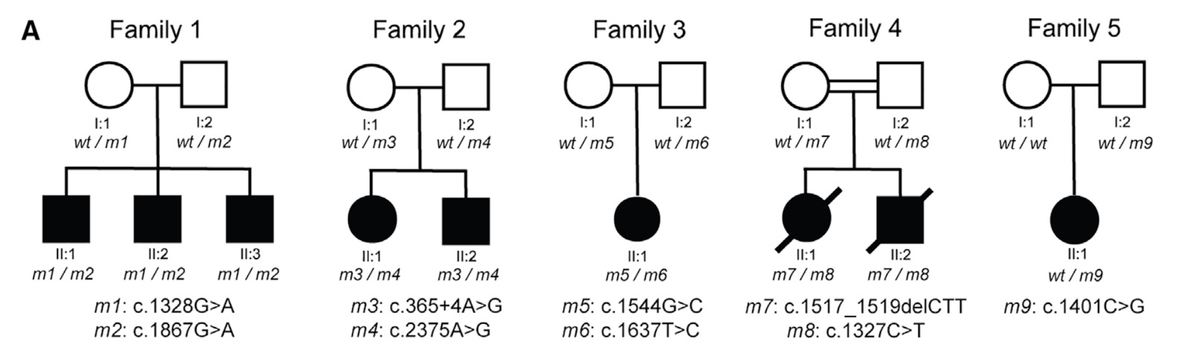
The first group of scientists, from Israel, published in PNAS their work on the genetic investigation of a consanguineous Bedouin kindred where multiple individuals suffered from a severe limb girdle muscle disease.

The disease manifested in the 4th decade of life, starting as a mild to moderate pain and fatigue in proximal and axial muscles that quickly progressed to severe weakness, often involving respiratory muscles. The patients became wheelchair bound and required assisted ventilation.
Through exome sequencing, the authors identified the genetic cause: a homozygous missense mutation within a highly conserved region of HMGCR that severely reduced the HMG CoA reductase’s affinity to its substrate HMG CoA.

The biallelic mutations reduced the function of the enzyme to a critically lower levels, but did not entirely abolish the activity. It makes sense, as complete deficiency of this enzyme is expected to be incompatible with life. Homozygous knockout of HMGCR is embryonically lethal in mice.
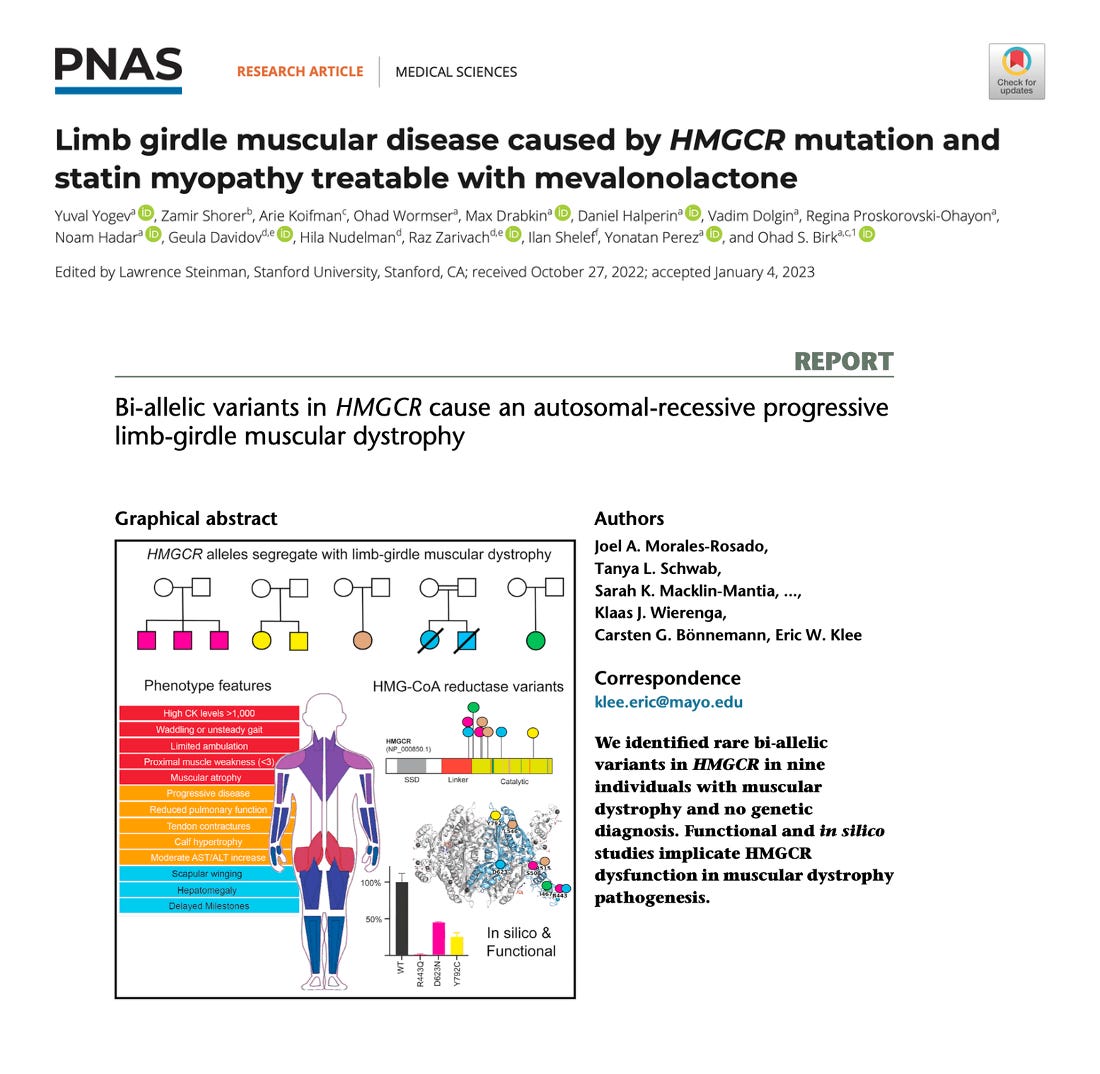
Similarly, the second team of scientists from the USA published in AJHG recently their work on the genetic investigation of nine individuals from unrelated families who all suffered from a limb-girdle like muscular dystrophy.
The patients had similar features as those from the Israeli study: gradually worsening proximal and axial muscle weakness leading to loss of ambulation and respiratory insufficiency, except that here disease onset was earlier, ranging from childhood to adolescence.
Exome sequencing revealed compound heterozygous missense variants in all the patients except one who, the authors speculate, might be a homozygous for a missense variant due to uniparental disomy.
All the identified missense variants were located within conserved residues clustering within protein domains critical for enzyme activity. In vitro assays confirmed defective enzyme activity at varying levels of severity.

But what is amazing about these discoveries is that scientists have not only established the precise cause of statin associated myopathy, but might have also found a treatment for it.
Going back to the Israeli study, the authors didn't stop at just diagnosing the genetic cause, they went one step further and ran an n=1 clinical trial. If the HMG CoA reductase deficiency is hurting muscles, then will mevalonic acid supplementation help halt the muscle damage and possibly reverse the symptoms?
The Israeli scientists received approval for the trial from the Israeli ministry of health under the compassionate treatment procedure and treated one of their patients with weekly oral dose of mevalonalactone. The doctors noticed improvement in muscle function as early as day 21. While previously the patient was unable to do any of these tasks, now she can raise herself sideways from sitting position, fully abduct her arm, extend her knees and feed her grand child, stand with assistance and breathe without ventilation. A supplementary video from the paper recorded 4mon after treatment, showing that the pt was able to abduct her arm fully, which wasn't able to before the treatment.
The authors also modeled statin associated myopathy in mice and demonstrate that mevalonolactone supplementation reverses statin induced myopathy.

The authors are currently extending the treatment to other patients and envision that mevalonolactone might become a standard treatment for statin-induced myopathy in the future. If this happens, all those who will benefit will owe it to these rare disease patients.

Cool, but wouldn't supplementing mevalonate be expected to cancel the cholesterol-lowering effects of statins?